Assessing wellbeing, safety and risk
Children and families need to be provided with timely and effective assessment to determine the factors affecting the safety and wellbeing of their children.
Assessment of safety and risk
Assessment is an ongoing holistic process that helps inform an understanding of the child’s immediate and ongoing safety, experiences and needs. The intent of an assessment is targeted, depending on what is happening for the child and family.
Children’s safety is always at the forefront when we are working with families. This means we seek to understand the child's daily lived experience to better understand how safe they are and how safe they feel. To ensure these assessments are thorough and well-informed, it is vital for all services supporting a family to share information and be involved in decision-making.
Triage assessment at the CSC
The triaging process helps to make sure that children at the highest risk are given priority to be allocated a field response. In a field response, a practitioner will make further assessment about the safety of the child and risk to the child. It is also an opportunity for those children who are unable to be allocated to a DCJ practitioner to be engaged with other services where possible.
The triage caseworker considers the reported concerns, supports already involved with the family, and other information known about the family to make a recommendation. Further information may be sought from other agencies or individuals to inform the triage recommendation. Through triage assessment, a decision is made to allocate, transfer, refer or close a report (within 28 days of being received at the Helpline).
If a report cannot be immediately allocated to a practitioner but needs a response, the matter can go to the CSC weekly allocation meeting or an Interagency Case Discussion could occur.
Triage assessment also occurs at the Joint Response Unit (JRU) as part of the Joint Child Protection Response Program, discussed below. When the Helpline sends a report to the JRU, the three agencies at the JRU (DCJ, Police and Health) undertake joint triage assessments to determine the most suitable referral pathway to address safety issues, health needs and policing response.
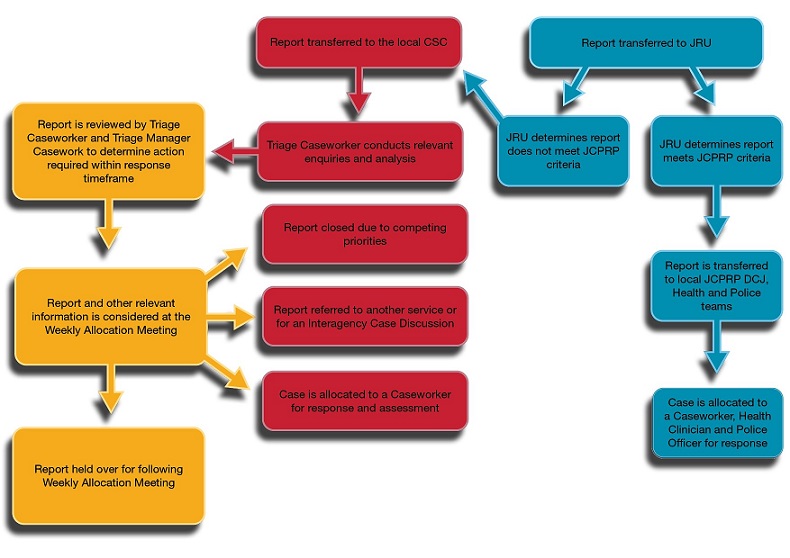
A text alternative to the Triage Assessment diagram is available.
Weekly Allocation Meeting
Weekly Allocation Meetings (WAM) at the CSC are chaired by the Manager Client Services (MCS) and attended by Managers Casework (MCW) and often the triage caseworker. WAM is a forum for the child protection leadership team to make a decision about the most appropriate outcome for each reported family.
The WAM decision about which family is the highest priority requires an understanding of the vulnerability and safety of children, features of neglect and abuse, and the possible outcomes to a child if the report is not allocated. This requires the consideration of:
- the history of the family
- factors impacting the child’s vulnerability
- support networks available for the family
- strengths and protective factors
- the types of reported abuse or neglect.
Information gathered and analysed by the triage caseworker is vital to informing the discussion and decisions at WAM.
Prior to WAM, the leadership team need to understand the capacity of the unit and local DCJ funded services to work with new families. This understanding can make sure the right families are provided the right service at the right time.
The MCS is responsible for approving all final decisions at WAM. These can include gathering further information, allocating for a response, referring to a service, closing the case file, an Interagency Case Discussion, or holding over for the next WAM. If a report cannot be allocated at WAM it can be held over for further review at the next WAM. A report can be closed after WAM without allocation if other reports are higher priority for allocation, or the report has remained unable to be allocated for more than 28 days.
Interagency Case Discussion
An Interagency Case Discussion (ICD) meeting can enable agencies supporting a family to share expertise and important, current information. Additionally, any actions or referrals to services that may be implemented with the family by the supporting agencies to reduce risk to the child or young person are able to be identified and discussed.
A DCJ practitioner invites representatives from relevant agencies and services to the ICD and chairs the meeting to facilitate information exchange and planning for the family.
Safety assessment, risk assessment and risk Re-assessment (SARA)
After the triage process, when it is agreed that a field response needs to occur to assess the safety and risk to a child, a family will be allocated a practitioner to complete a SARA. Safety assessment assesses the child’s present danger and the interventions currently needed to protect the child. Risk Assessment looks at the likelihood of future involvement with child protection authorities.
Assessment of child safety and risk relies on respectful engagement with the family. It brings together all that we know about the family and links this to our professional experience, knowledge and theory.
It is important that dangers and risks are explained to families, that we are specific about these concerns, and what families need to change, to ensure their child/children are safe.
Safety assessment
The safety assessment helps practitioners determine the immediate safety needs of the child and if they may safely remain in the home, with or without a safety plan in place. To do this, practitioners consider the vulnerabilities of the child, assess and determine if there are immediate or imminent dangers in the household, and assess the protective abilities of the parents.
If a danger is identified, the protective abilities are then used to develop a safety plan with the family to ensure the safety of the child. In most instances, it is not safe to rely only on the person causing the danger to mitigate the dangers found in a safety assessment. Therefore, the safety plan should use the support of other family or community members who are able to act to support the parents to protect the child.
In circumstances where a danger is identified and no parental protective abilities can be determined, the child will be considered ‘unsafe’ in the home and alternative care arrangements must be made.
Risk Assessment
Within 30 days of completing a safety assessment practitioners complete a risk assessment. This estimates the likelihood of future child protection system involvement. It assists practitioners to determine which cases should be continued for ongoing services and which may be closed at the end of the investigation.
The risk assessment requires consideration of:
- the child’s prior history of abuse and neglect and how they experienced this
- the parent’s pattern of behaviour placing children at danger or risk
- the parent’s own childhood experiences of abuse and neglect
- the parent’s resistance and prior strengths when managing mental health, drug abuse or domestic violence
- analysis of the effectiveness of previous casework the family has experienced, whether the interventions put in place increased safety for the children, and whether or not they were culturally appropriate
- the parent’s attitudes to the current abuse or neglect concerns.
To gather this information the practitioner will speak with the children, parents, extended family members, and other services involved with the family. The practitioner may also undertake consultation with an Aboriginal or multicultural practitioner or community member, a DCJ Psychologist and/or a Casework Specialist. The Aboriginal Consultation Guidecan be used to guide effective and ongoing consultation with Aboriginal families and communities.
It may be necessary for the practitioner to conduct specialised consultation with children and parents with disability. Generic approaches will not always be sufficient to ensure their safety and wellbeing.
The risk assessment can have an outcome of low, moderate, high or very high risk. Families with no identified dangers and low or moderate risk are determined not to require ongoing casework. Their cases are closed by DCJ, sometimes after being referred to other services for support. Other families require intervention from DCJ or a non-government organisation to reduce the level of risk or ongoing dangers to the child.
Family Action Planning
A quality case plan creates purposeful and meaningful opportunities for sustainable change in families which helps to keep children safe.
Family Action Plans are case plans for change that are developed in partnership with families and their support network to address concerns and worries for children. Supporting parents to take ownership of the changes needed, we will be able to increase child safety.
The focus of Family Action Plans is to influence change until the risk level comes down and it is safe for children to stay safely at home.
Family action planning involves:
- creating a future vision of family safety
- building a shared agreement of what needs to change
- stepping out the actions needed to achieve that change
- engaging and connecting with support services (based on how ready the family is) to assist in those steps
- measuring progress towards a goal.
Risk Re-Assessment
Within 90 days of first visiting a family, practitioners will complete a Risk Re-Assessment. This assessment helps the practitioner determine when risk has been reduced sufficiently so that the case may be recommended for closure. To inform this assessment, the practitioner will:
- Regularly speak with each child to understand their experiences and listen to their concerns
- Regularly observe each child in their home environment interacting with family and other household members
- Check in with how the family is progressing against the case plan goals and what barriers may be impacting on their progress
- Continue to seek information from a range of sources both formal and informal, such as important people in the family networks, and government and non-government agencies.
The outcome of the risk re-assessment can be low, moderate, high or very high. If the level of risk to the child has been reduced to low or moderate (and there are no unresolved dangers), the case will be closed. If the risk remains high or very high, or there are unresolved dangers, casework with the family will continue. For families with successive high or very high risk re-assessment outcomes, more intrusive intervention may be considered to reduce the level of risk to the child.
For legal options to address dangers and reduce risk Refer to Courts Involving Children and Young People (insert hyperlink ).
Review or closing Safety Assessment
Review of safety assessments are required when circumstances change or when new ROSH information is received about the family. A case cannot be closed unless the most recent Safety assessment outcome is ‘safe’.
Open child protection cases involving a parent(s)/carer(s) with a known and current diagnosis of a severe or persistent mental health issue are not to be closed prior to consultation about the closure with key mental health services involved with the family.
Restoration Assessment
Within 90 days of the Family Action Plan for Change being developed where the goal is restoration, practitioners will complete the restoration assessment. This is applied for families with a child in out-of-home care with a goal of ‘restoration’, or ‘determine permanent care’ every 90 days until it is safe for the child to be returned home. This assessment helps the worker assess when it might be safe for the child to be returned to the home, or when a change in permanency goal should be considered. This tool focuses on assessing risk, suitability of family time, and progress towards the case plan.